
Summary
These tables provide information on mental health and addiction service use for the 2015/16 financial year (1 July 2015 to 30 June 2016) and highlight notable trends between 2001/02 and 2015/16. An overview of key findings can be found at the bottom of this webpage and in the accompanying spreadsheet containing the tables.
The tables include information on mental health and addiction services (care) provided by secondary organisations funded by the Ministry of Health. Specifically, these tables cover: demographic and geographic information, client referral pathways, the types of services provided, the outcome of the services and legal status and diagnosis information.
The tables do not include information on:
- the provision of primary mental health care, such as care provided by general practitioners
- secondary mental health services funded by other government departments e.g. funded by the Ministry of Social Development
- problem gambling
- people with a mental illness who do not access services.
The information was sourced from the Programme for the Integration of Mental Health Data (PRIMHD pronounced ‘primed’). The data was collected by district health boards (DHBs) and non-governmental organisations (NGOs).
Data quality and interpretation notes
The Ministry of Health, DHBs and NGOs are actively engaged in reviewing and improving the quality of PRIMHD data, but because there are some known issues yet to be addressed, numbers should be interpreted and reused with due consideration and care. Although it is not practical to record all known data quality issues on this webpage, the most important considerations have been detailed below. If you need further detail please contact [email protected].
Under-reporting of data
Some organisations had breaks in reporting and/or incomplete data in PRIMHD in the 2015/16 year. A few NGOs started and/or stopped reporting during 2015/16 so not all organisations have data for the whole time period. It is known that Southern District Health Board's PRIMHD data is under-reported for the 2015/16 year, so figures may be low in these data tables. For this reason please use Southern's data with caution.
Coding changes may cause artificial variance and trends
Observed variance and trends may be a result of differences in coding practices across service providers and time, for example, coding changes have influenced the number of crisis contact services reported by some DHBs.
To assist with activity (a synonym for services and care) coding in particular, the Ministry of Health published a Guide to PRIMHD Activity Collection and Use in early 2016. We suggest you consult this guide to aid interpretation. A high level description of each of the activity types can also be found within the PRIMHD Codeset.
Increased NGO reporting will influence trends
In 2008, DHBs began reporting to PRIMHD. In addition, from this date an increasing number of NGOs began reporting to the PRIMHD database. Shifts or patterns in the data after 2008 may reflect the gradual adaptation of non-governmental organisations into the PRIMHD collection in addition to, or instead of, any trend in mental health service use or outcomes. This point is illustrated by the artificial trend within the chart below in which the crude rate of clients seen by NGOs in 2015/16 was eight times that reported in 2008/09. Although NGO data is still incomplete, the Ministry of Health considers it complete enough for comparison across time from 1 July 2012 onwards.
Crude rate of clients seen by NGOs, 2008/09 to 2015/16
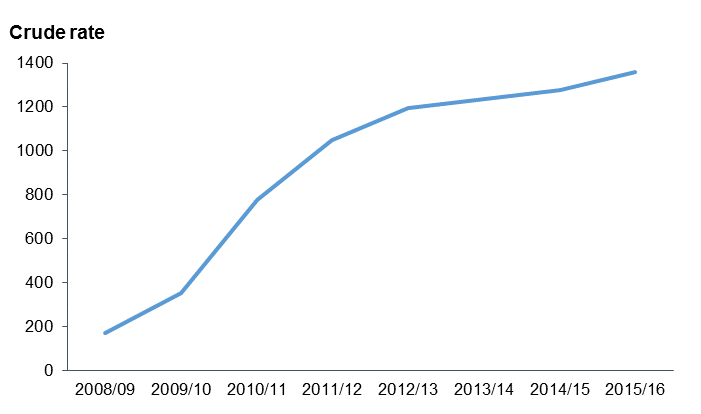
Notes:
- Crude rate is per 100,000 population.
- All organisation types apart from district health boards have been included in the non-governmental organisation category. This includes charitable trusts and a very small number of private hospitals.
Completeness of data for older people
Mental health and addiction services for older people are funded as mental health and addiction services in the Northern and Midland regions. In the Southern and Central regions they are funded as disability support services. PRIMHD mainly captures mental health and addiction services, and occasionally captures data on disability support services. This means data on healthcare users aged over 65 (including psychogeriatric services) is incomplete.
Data in these tables is not directly comparable to data in other reports
For several reasons the numbers in the tables are not directly comparable with the numbers in the Office of the Director of Mental Health (ODMH) Annual Reports, amongst other reports. The ODMH reports are published for a different purpose and use a slightly different method to identify the report subject matter. Further to this the OMDH reports are for a different time period and occasionally include manual data submitted by DHBs.
Data is continually updated and revised
The Ministry of Health is actively engaged in reviewing and improving the data quality of PRIMHD. PRIMHD is a living data collection, which continues to be revised and updated as data reporting processes are improved. For this reason, previously published data may be liable to amendments. Caveats under each table should be taken into consideration before any comparison is made. In particular, there was notable change made to the coding of team types as part of the HISO review of the PRIMHD Codeset. Team type data, extracted before 1 July 2014, should not be compared with the data within these tables.
To function as a national collection, PRIMHD requires integration with a wide range of patient management systems across hundreds of unique service providers. The quality and accuracy of statistical reporting relies on consistent, correct and timely data entry by the services that report to PRIMHD. As the services adjust to PRIMHD, it is expected that the quality of the data will improve.
Errata
These tables were updated on 27 February 2020. Seclusion data has been removed from these tables. An error was discovered in the way seclusion events were calculated. This error led to an undercount of seclusion events. We are in the process of publishing revised seclusion data that will be available in a stand alone dataset. For more information please contact: [email protected].
Key findings
Demographics
In 2015/16, a total of 171,033 clients were seen by mental health and addiction services. Of these, 89,379 (52.3%) were male, and 81,654 (47.7%) were female.
There were 142,039 clients seen by DHBs and 63,682 clients seen by NGOs. Some of these clients were seen by both DHBs and NGOs.
In 2015/16, the rate of Māori seen by DHBs was 4829.0 per 100,000 Māori population, a rise of 72.1% since 2001/02. In contrast the rate of non-Māori seen has risen more slowly (36.8% over the same time period).
Services provided in 2015/16
The most common type of team providing services to DHB clients was community teams, while the next most common team type was alcohol and drug teams. These two teams were also the most common team types providing services to NGO clients.
Activity type
In 2015/16, the most common type of activity (or service) provided by DHBs was ‘individual treatment attendances: family not present’. The most common type of activity provided by NGOs was ‘community support contacts’.
Deprivation
People living in the most deprived areas of New Zealand were 2.7 times more likely to be seen by mental health and addiction services than people living in the least deprived areas.
Long-term clients
As at 30 June 2016, there were 32,858 long term clients that were seen by mental health and addiction services for one year or more. Out of these clients, 21,111 were seen for two years or more.