

2026/27 Vote Health funding compared to 2025/26
Total Vote Health funding in 2026/27 is $33.031 billion, compared with $30.476 billion at the start of 2025/26, representing an uplift of $2.556 billion (8.4%). Total operating funding has increased by $1.571 billion (5.7%), compared with operating funding at the start of 2025/26.
In 2026/27, Health New Zealand’s funding for services is $27.154 billion. This is split across three appropriations: Hospital and Specialist services ($15.995 billion), Primary, Community, Public and Population Health Services ($10.348 billion) and Hauora Māori ($0.811 billion). This represents an increase of $1.525 billion (6%), compared with funding for services across these three appropriations in 2025/26.
The comparisons between 2026/27 and 2025/26 are based on total funding at the start of each respective financial year. They account for the removal of the requirement for Health New Zealand to pay a capital charge to the Crown in the coming financial year, by excluding the funding provided for this purpose in the 2025/26 year. The comparison excludes any funding set aside in tagged contingencies.
For details of factors that have an impact on the level of funding in Vote Health appropriations, please refer to the Supplementary Estimates of Appropriation for 2025/26 and Estimates of Appropriations for 2026/27. Both documents provide, for each appropriation, a detailed reconciliation in the ‘Reasons for Changes for Appropriation.’
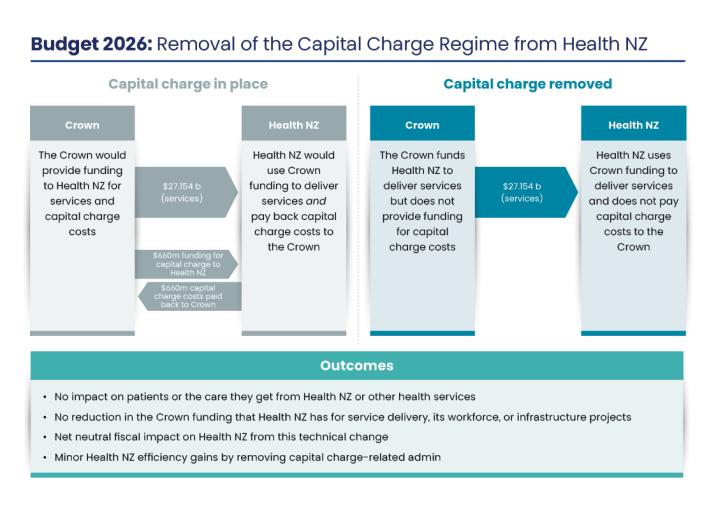
Further information on the change to the capital charge regime is provided below.
Capital charge regime
From 1 July 2026, Health New Zealand will no longer be required to pay a capital charge to the Crown. This is a technical change that will have no impact on overall funding for service delivery, infrastructure or patient care.
The capital charge regime pre-dates the 2022 health system reforms, when every district health board was required to pay capital charge twice a year based on their net assets position at the time.
Because Health New Zealand was previously funded to pay the capital charge but is no longer required to do so, the corresponding amount has been removed from Health New Zealand’s baseline. This has a net neutral fiscal impact on Health New Zealand and does not represent a change in the funding Health New Zealand has available to deliver services or develop infrastructure, and it will not impact patients.
Vote Health as a proportion of Gross Domestic Product
As a proportion of Gross Domestic Product (GDP), Vote Health varied between around 5.3–5.6% in the period 2000–2022, rising to 6%-7% post-COVID. It is projected to be around the top of that range in 2026/27.
Core Crown health funding
Core Crown health funding is $34.196 billion in 2026/27, compared with $32.133 billion in 2025/26. These totals include operating funding across Vote Health, disability support services and health payments to ACC. They exclude capital funding.
International comparisons
While comparing data between countries can be complex, the latest OECD publication, Health at a Glance, shows that New Zealand is generally in line with the OECD average in health spending as a percentage of GDP and health spending per capita.
The OECD data covers health expenditure, categorised and defined according to a System of Health Accounts. It goes broader than Vote Health to include other Government expenditure (such as ACC, or health spending in Corrections facilities), as well as privately financed spending (for instance, private health insurance).
Comparing data between countries can be complex because of differences in the way countries run their health systems and collect information. We are strengthening our data collection to improve the comprehensiveness of the information provided to the OECD on New Zealand’s health expenditure.