

On this page
-
…
What is the Global Burden of Disease study?
The Global Burden of Disease (GBD) study is a comprehensive global effort to quantify health loss from major diseases, injuries, and risk factors for 204 countries and territories. It is coordinated by the Institute for Health Metrics and Evaluation (IHME) based in the state of Washington, USA. The GBD study began in the early 1990s and now provides estimates of health loss for 371 diseases and injuries, and 88 risk factors. Further information can be found on the IHME website.
National level estimates for Aotearoa New Zealand have been provided annually by the GBD study since 2016. This is the first time the GBD study (2021) has also produced estimates of health loss for Māori in New Zealand. The inclusion of Māori and non-Māori estimates was requested to provide a better understanding of health trends and health loss for Māori to add to the existing knowledge base of Māori health outcomes.
The report Māori Years of Life Lost: Estimates from the Global Burden of Disease Study, 2021 provides estimates and an analysis of the years of life lost (YLL) for Māori.
How to position the use and interpretation of Māori GBD estimates
Māori GBD estimates should be understood alongside existing information on the enduring health inequities experienced by Māori and with consideration of the determinants of health. Below we provide guidance on how the data can be used in a culturally safe way to inform health outcomes for Māori.
The use and interpretation of data supplied by the GBD study should adopt a strengths-based approach, which firmly rejects ‘victim-blame’ or ‘cultural-deficit’ interpretations. It is crucial to understand that identifying inequities between Māori and non-Māori does not imply Māori failure or shortcomings (Curtis 2016). Instead, a Kaupapa Māori perspective highlights racism, privilege, and power imbalances as fundamental drivers of ethnic inequities in health for Māori compared to non-Māori (Curtis et al 2023).
Wider determinants, such as social and economic factors, experiences of discrimination, and the ongoing impacts of colonisation, are crucial considerations in Māori health. A useful model for understanding the determinants of health and positioning the use and interpretation of the Māori GBD estimates is the Te Kupenga Hauora Māori model for explaining indigenous/ethnic determinants of health (Curtis et al 2023). This model emphasises the importance of a holistic approach to Māori health, incorporating cultural, social, and environmental factors. This model advocates for the protection, promotion, and improvement of Māori health to achieve equity in health outcomes and build towards pae ora (healthy futures) for Māori.
Things to consider when using the estimates
Terminology and worldviews
The GBD study is based on a biomedical model and does not consider the role of the determinants of health within the context of New Zealand, nor does it consider Māori perspectives of health. The determinants of health are a range of factors that influence people’s mental and physical health, such as the circumstances and environment in which people are born, grow up, live, learn, work and age. These factors include social and economic conditions, experiences of discrimination, access to healthy environments and the ongoing impacts of colonisation. Different exposures to these determinants between groups of people can cause health inequities and disparities. This report should be interpreted alongside Māori health models and take into consideration the societal, environmental, and cultural contexts unique to New Zealand.
Definitions of disability
The definition of disability used by the GBD study is different to the definition of disability currently used in New Zealand, which is based on the Social Model of Disability. The New Zealand Disability Strategy (2016-2026) uses the United Nations Convention disability definition: ‘…those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others…’ (Whaikaha 2024). The term ‘disability’ in the GBD estimates refers to any short-term or long-term health loss, or less than ‘ideal’ health. Disability results when people with impairments are exposed to unaccommodating environments, ie, it is society that is disabling.
We acknowledge that the term 'disability' itself is a deficit-framed term and is not consistent with Te Ao Māori worldviews, nor aligned with mana-enhancing terminology. Te Ao Mārama Aotearoa (the national peak body representing Disabled Māori) advocates for the use of the term ‘Tāngata Whaikaha Māori’, which means ‘people who are determined to do well’ (Ministry of Health 2018b).
Estimates and modelling assumptions
All GBD data are estimates that are calculated using statistical modelling. In some cases, assumptions are made based on the data that is available. These assumptions often represent non-population-specific realities and may not reflect the experiences or realities of Māori.
The strength of the GBD project is that it produces cause-specific estimates of diseases, injuries, and risk factors. However, the quality of these estimates relies on the quality and coverage of the data. Statistical modelling techniques account for gaps in the data, but there is still a level of uncertainty that varies for each disease, injury, and risk factor, and consequently for the various measures (described below).
The disability definition used for the GBD impacts the Years Lived with Disability (YLD) measure, as it is calculated by multiplying cause-specific prevalence by the respective disability weights. The GBD includes short-term health loss and less than ‘ideal’ health as disability, because they are estimating the number of years lived in less-than-ideal health. Therefore, this difference needs to be considered when interpreting YLD estimates as the GBD disability definition is broader than that used in New Zealand.
Ethnicity data quality
The ethnicity data provided to the IHME for modelling comes from multiple sources. Cause specific ethnicity data is from the National Health Index (NHI - sourced from hospitals and primary health organisations), population data is from the census held by Stats NZ, and ethnicity information for causes of death is sourced from the register of deaths held by the Department of Internal Affairs. Ethnicity information is different between these sources as health providers do not collect it in the same way as the census and the register of deaths, which creates discrepancies that are larger for Māori and those with more than one ethnicity (Blackmore et al 2024; Tan et al 2010). This leads to undercounting of Māori in health data, which needs to be considered when interpreting the results.
Additionally, GBD estimates are available from 1990-2021, but usage should focus on Māori estimates from 1996 onwards. Prior to this period the quality of ethnicity data was unreliable, and Māori were often undercounted due to different definitions of ethnicity on death registration, birth registration, and census forms.
Comparing Māori to non-Māori
GBD estimates have been provided for Māori and non-Māori. Prioritised ethnicity is used in health data, which categorises a person into a single ethnic group based on the Health Information Standards Organisation Ethnicity Data Protocols. As Māori are prioritised first, an individual who identifies with multiple ethnicities, including Māori, is categorised as Māori.
This ethnic breakdown creates the opportunity to look at Māori specific estimates, and to compare them against non-Māori. Using non-Māori as a comparator for health outcomes can mask disparities by masking differences in the non-Māori group. For example, Pacific peoples often have similar health outcomes to Māori, which can be different to health outcomes for people in the Asian or European/Other ethnic groups.
Age-standardisation
The risk of developing chronic diseases increases with age. This is important to consider when comparing disease rates between population groups with different age structures. The Māori population has a younger age structure than the non-Māori population, so comparing observed (crude) rates can mask differences between these two populations.
Age-standardisation is a method used to account for the differences in age-structure between populations. It involves adjusting the crude rates to a ‘standard population’ with a specific age structure and the rates will differ depending on the standard population used. The standard population used by the IHME to age-standardise the estimates was made to allow comparisons across all countries and jurisdictions that participate in the GBD study, the method for which is described in this paper on demographic analysis for the GBD Study.
Caution is advised when comparing age-standardised rates from the GBD study with those in publications that use a different standard population. This includes Health New Zealand web tools that use the WHO World Standard Population and publications such as Tatau Kahukura: Māori Health Chart Book that use the 2001 Māori census population, as recommended in the position paper on Māori health analytics – age standardisation (Ministry of Health 2018a).
The Māori health estimates that have been released
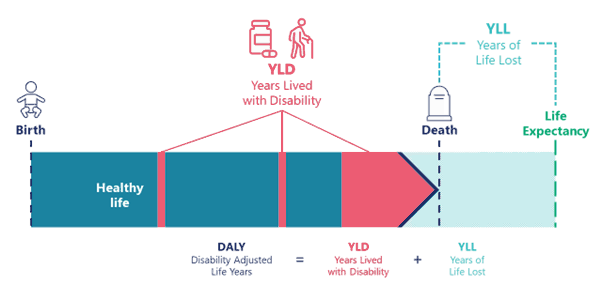
The GBD produces regular estimates describing life loss and health loss. Figure 1 below shows the standard GBD metrics released each cycle, and how they relate to each other across a person’s lifetime.
Figure 1: Diagram of the GBD metrics and how they relate to each other
Data available on the GBD site
The 2021 GBD metrics produced for Māori are outlined below. For more detail on each metric and how they are estimated, see the GBD protocol guide. All metrics are released for Māori and non-Māori as numbers, crude and age-standardised rates, proportions and percentages, by age and sex, and for every year from 1990-2021.
Years of life lost
Years of life lost (YLL) is the number of years of life lost due to premature mortality (early death). YLL is calculated by subtracting the age at death from the longest possible life expectancy for a person at that age. This is done for each cause of death to provide an understanding of the impact that diseases and injuries have on premature mortality in a population. The life expectancy measure used is at the global level to allow comparisons between countries, it is constructed using the lowest observed age-specific mortality rates across all locations with a population of more than 5 million.
Years lived with disability
Years lived with disability (YLD) is the number of years of life lived with any short-term or long-term health loss, which can also be described as years lived in less-than-ideal health. This measure provides an understanding of the impact of different diseases and injuries on quality of life.
YLD measures are estimated by taking the prevalence of the condition multiplied by the disability weight for that condition.
Disability weights
Disability weights represent the severity of a disease and range from 0 (perfect health) to 1 (equivalent to death). Disability weights are assigned to each health condition included in the GBD and are based on surveys that used pair-wise comparison methods in which respondents were asked to indicate which of two health states they considered to be ’healthier’. Four surveys were conducted in low- and middle-income countries, four internet surveys conducted in multiple European countries, one telephone survey in the USA, and one open-access online survey conducted globally to provide pair-wise comparisons. Disability weights were then derived from these comparisons and given numerical values.
Disability-adjusted life years
Disability-adjusted life years (DALY) are the number of years of healthy life lost to premature death and disability (health loss). Disability is defined by the IHME as short-term or long-term health loss, or less than ‘ideal’ health, this definition differs from the functional view of disability. DALY are estimated by adding YLL to YLD.
DALY estimates provide a more complete overview of the health burden of different diseases and injuries by combining the impact of both premature death and health loss.
Life expectancy
Life expectancy (LE) is the number of years a person is expected to live at a given age, assuming they will experience the age-specific mortality rates observed each year throughout their lifetime. LE at birth is the age a person is expected to live when they are born. The LE for an age group, is determined from the first year in the age range.
This metric reflects overall population health and how well the health system is reducing premature death.
Deaths
The number or rate of people who die each year from all-causes or from a specific cause.
The IHME classifies 371 causes of death, with descriptions based on groupings from the relevant International Classification of Disease (ICD 10th edition) codes.
Incidence
Incidence is the number of new cases of a given condition or disease during a given period in a specified population. It is differentiated from prevalence, which refers to all cases, new or old, in the population at a particular time.
Incidence can be useful when analysing trends in new cases of a particular condition or disease over time.
Prevalence
Prevalence is the number of people in a population who have a condition or disease at a given time. It is different from incidence as it takes into account the people who already had the condition, new cases, and any deaths in the population.
Prevalence is used when analysing trends in all current cases of a particular disease or condition.
Risk-attributable deaths or DALYs
The share of deaths or DALYs that can be attributed to – ie, estimated to occur due to – exposure to a particular risk factor (eg, alcohol-attributable deaths, or deaths attributable to air pollution, etc). This can tell us what risks are associated with a particular condition or disease.
Health-adjusted life expectancy
Health-adjusted life expectancy (HALE) is the number of years that a person at a given age can expect to live in good health, if the rates of all-cause mortality and all-cause disability in a specified year of interest remain constant into the future. While life expectancy summarises a population’s mortality experience, HALE uses the same concept, but adjusts years lived at each age by the probability of health loss. The average amount of health loss a person experiences increases with age, as disability generally also increase with age, so HALE adjusts downwards those remaining years of life more for older people than for younger people.
Uncertainty intervals
The uncertainty interval tells us how certain or accurate the estimate is. It is a range of values that reflects the certainty of an estimate. Larger/wider intervals with more uncertainty can result from limited data availability, small studies, and conflicting data, while smaller/narrower uncertainty intervals can result from extensive data availability, large studies, and data that are consistent across different sources.
Causes and levels
Each of the GBD estimates are broken down by causes of health loss – referring to diseases and injuries. The full list of causes (diseases and injuries) included in the GBD study can be found at: GBD data and tools guide.
The 371 causes of health loss studied within the GBD are arranged in hierarchical nested categories – referred to as ’levels’ – within the GBD ‘cause lists’. Level 1 is the broadest category, and with each subsequent level the causes of health loss are broken down with increasing specificity.
How to access the data
The results have been made available online in the IHME data tools.
- The GBD 2021 Compare tool. This tool has many visualisations to compare trends in diseases, injuries, and risk factors.
- The GBD 2021 Results tool. With this tool you can select, filter, view, and download the data.
Appendix 1: Relationship between the Ministry of Health and Institute for Health Metrics and Evaluation
The Ministry of Health has a long-established relationship with the Institute for Health Metrics and Evaluation (IHME) in working together to provide regular releases of national-level GBD estimates for New Zealand. In May 2024, the Ministry of Health announced the release of the 2021 national estimates. The latest national-level estimates are available here: GBD compare tool.
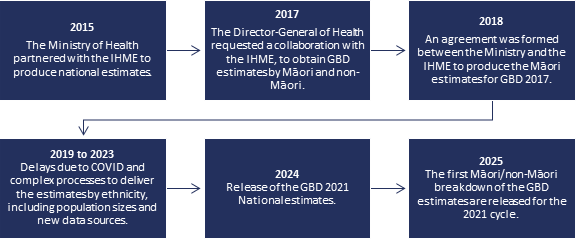
The diagram below provides an overview of the timeline leading up to the release of the GBD estimates for Māori.
Figure S1: Timeline of the relationship between Ministry of Health and IHME
Text description
2015
The Ministry of Health partnered with the IHME to produce national estimates.
2017
The Director-General of Health requested a collaboration with the IHME, to obtain GBD estimates by Māori and non-Māori.
2018
An agreement was formed between the Ministry and the IHME to produce the Māori estimates for GBD 2017.
2019 to 2023
Delays due to COVID and complex processes to deliver the estimates by ethnicity, including population sizes and new data sources.
2024
Release of the GBD 2021 National estimates.
2025
The first Māori/non-Māori breakdown of the GBD estimates are released for the 2021 cycle.
Partnering with the IHME to produce health-loss estimates benefits the Ministry by gaining access to their well-established and well-resourced international methodology. Producing these estimates is complex and time consuming. Previously, the Ministry has produced their own estimates for the total population and for Māori. The first New Zealand burden of disease and injury study was published in 2001. It was based on 1996 data and included estimates for Māori. The second report published in 2013, based on 2006 data had projections to 2016 and included estimates for Māori (Ministry of Health 2013).
This 2021 GBD cycle is the first to publish GBD estimates for Māori, and the first attempt at applying the GBD framework to an indigenous population globally. A potential wider implication of providing the GBD estimates for Māori is creating a drive for other jurisdictions with indigenous populations to obtain ethnic breakdowns of their national GBD estimates. Consequently, the indigenous health evidence base will be strengthened, and opportunities will be created in the future for greater international collaboration to address health inequities.
References
Blackmore B, Elston M, Loring B, et al. 2024. Accuracy of ethnicity records at primary and secondary healthcare services in Waikato region, Aotearoa New Zealand. The New Zealand Medical Journal 137(1602): 111–24.
Curtis E. 2016. Indigenous positioning in health research: The importance of Kaupapa Māori theory-informed practice. AlterNative 12(4): 396–410.
Curtis E, Jones R, Willing E, et al. 2023. Indigenous adaptation of a model for understanding the determinants of ethnic health inequities. Discover Social Science and Health 3(10): 10.
Ministry of Health. 2013. Health Loss in New Zealand: A Report from the New Zealand Burden of Diseases, Injuries and Risk Factors Study, 2006–2016. Wellington: Ministry of Health.
Ministry of Health. 2018a. Position Paper on Māori Health Analytics – Age standardisation. Wellington: Ministry of Health.
Ministry of Health. 2018b. Whāia Te Ao Mārama 2018 to 2022: The Māori Disability Action Plan. Wellington: Ministry of Health.
Tan L, Blakely T, Atkinson J. 2010. Ethnic counts on mortality and census data 2001–06: New Zealand census-mortality study update. New Zealand Medical Journal 123(1320): 37–44.
Whaikaha. 2024. New Zealand Disability Strategy. Wellington: Ministry of Social Development.